.svg)


A New Role for CMOs in Fixing Documentation Fatigue
Documentation fatigue is no longer a CDI problem. It is a leadership problem. And CMOs are being asked to solve it with tools that were never designed to fix the root cause.
Clinical documentation queries have become distracting and increasingly disconnected from clinical reality. What began as a well-intended effort to improve severity capture has, in many organizations, evolved into a stream of retrospective questions that rarely change documentation behavior in real-time.
For Chief Medical Officers, this has created a difficult tension:
Support documentation initiatives that finance, quality outcomes, and compliance depend on, or advocate for physicians who feel burned out by a process that often lacks clinical clarity and consistency.
Until now, there has been no objective way to resolve that tension. Our CMOs appear to be stuck between a rock and a hard place.
Queries are the symptoms.
Variation is the disease.
Until variation in how clinical conditions are defined, prioritized, and documented is addressed at the source, documentation fatigue will persist — regardless of how sophisticated the tools become.
The Real Reason CDI Exists: Unmanaged Clinical Variation
At its core, CDI exists for one reason: variation. Variation in:
- How physicians define clinical conditions
- How consistent conditions are documented
- Which diagnoses are prioritized amid competing clinical and organizational demands
- How documentation is interpreted by reviewers, coders, or algorithms
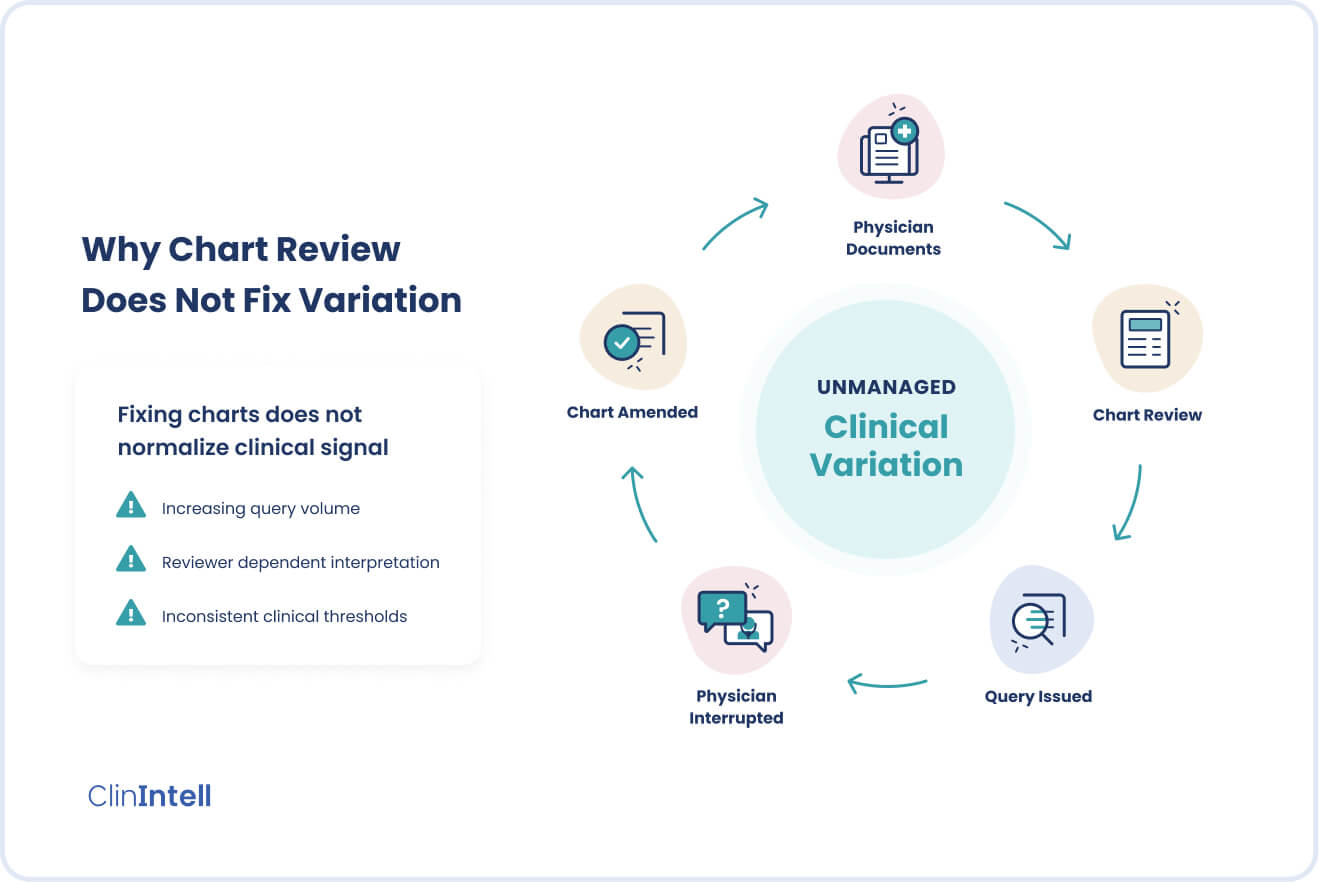
Traditional CDI has attempted to manage this variation “after the fact” by reviewing charts and issuing queries when documentation appears incomplete or ambiguous.
But this approach never addresses the root problem. Remember, the queries are only the symptoms of the real problem, which is variation. Physicians document based on their own mental models, definitions, and priorities — not a shared, population-informed or strategy-driven standard.
As a result, “CDI” becomes reactive and noisy, and trust with physicians erodes over time. This environment has created demand for tools that promise to eliminate queries by prompting physicians in real-time. While appealing in theory, this simply shifts the disruption — from retrospective CDI queries to in-workflow interruptions.
In practice, real-time prompts surface when the system is ready, not when the physician is clinically synthesizing the diagnosis. The interruption remains. Only the timing changes. While designed to reduce cognitive burden, many real-time tools struggle to integrate naturally into clinical reasoning and may introduce additional signals into an already complex workflow.
For example, a physician managing a patient with sepsis may prioritize stabilization, antibiotics, and organ support early on. A documentation prompt asking whether “sepsis with acute organ dysfunction” is present may surface hours later — not at the moment the physician is clinically synthesizing the diagnosis, forcing a mental shift that feels administrative rather than clinical. The same dynamic occurs with conditions like acute respiratory failure or acute kidney injury, where clinical recognition and decision making precede documentation accuracy.
The underlying issue remains unresolved — clinical condition reporting practices are not being aligned or standardized at the source with physicians diagnosing patients. Without addressing variation in how condition thresholds are defined, prioritized, and documented, neither retrospective queries nor real-time prompts can deliver sustainable improvement.
Why Queries Can’t Fix the Variation Problem
All chart-based CDI approaches (manual, AI-assisted, or consultant-led) depend on clinical information that already exists in the medical record.
Queries can only be compliantly issued if:
- There is sufficient documentation from the source (provider) to suggest a diagnosis
- The diagnosis is clinically significant
- The reviewer or technology interprets the chart correctly
- The opportunity is visible within a single encounter
If documentation practices vary, and we know they always do, the system cannot normalize performance. It simply flags inconsistency after it occurs.
Over time, this leads to:
- Increasing query volume
- Persistent variation across physicians and services
- Minimal improvement in documentation practices
- Diminishing returns in CMI and risk adjustment
- Escalating physician disengagement
This is why the industry has hit a wall. Despite increasing CDI investment, variation across physicians often remains unchanged year over year.
Why CMOs Have Been Forced into a Defensive Position
Physicians and physician leaders alike have long raised concerns that CDI queries are inconsistent and disconnected from clinical reality.
CMOs have historically lacked the data to determine whether queries reflect true population-level gaps or simply reinforce variation. As a result, their long-term impact on documentation best practices has been minimal.
Chart-based assessments are inherently sample-driven and reviewer or technology-dependent, and while they measure what could have been queried, they are unable to measure whether clinical documentation practices are becoming more consistent and aligned with true severity across the population.
Normalizing Clinical Signal Across the Population
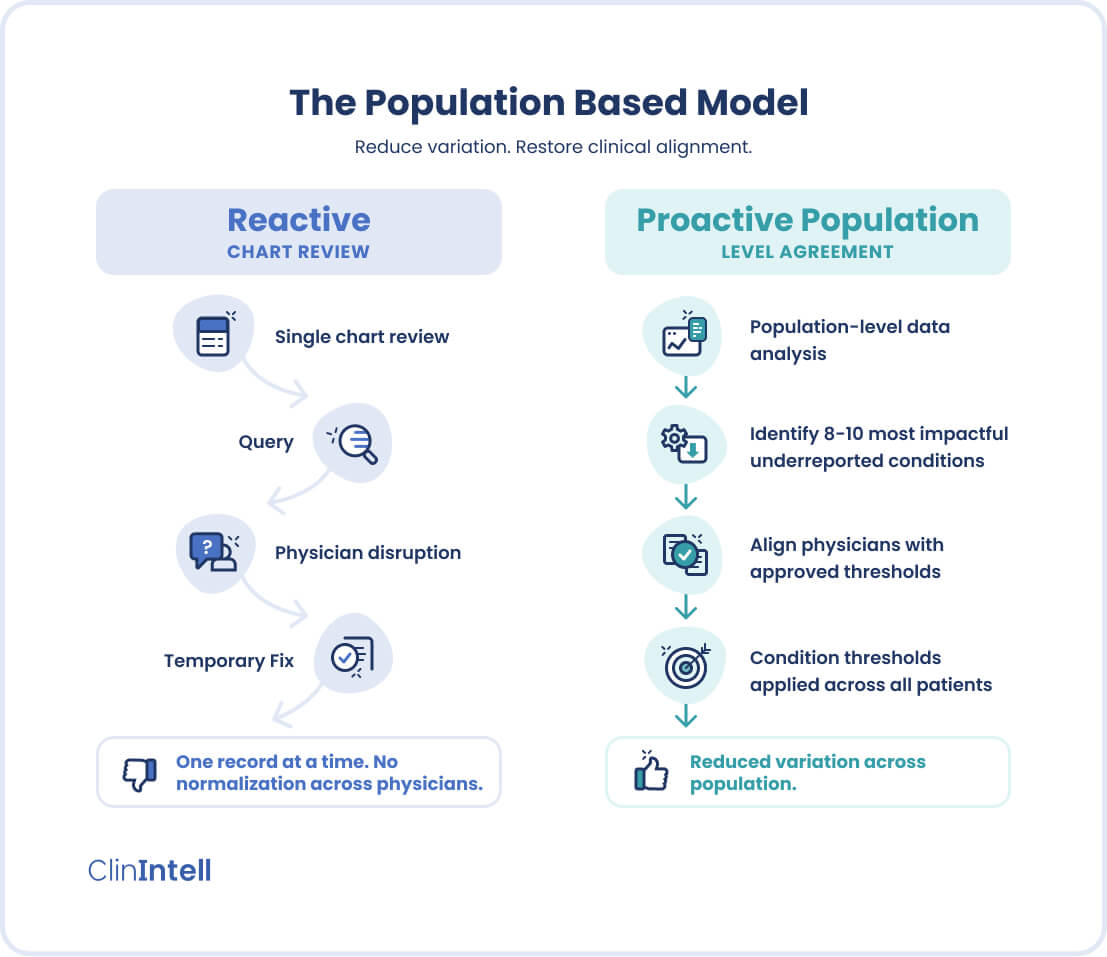
ClinIntell’s Population-Based Assessment starts from a fundamentally different place.
Instead of searching charts for missed diagnoses, ClinIntell evaluates high-impact clinical signals across the entire inpatient population, using claims-level data over time. Physicians have become desensitized to these clinical signals, while CDI and other review approaches rely on them for the generation of queries. Once a short list of high-impact clinical conditions has been identified as being under-reported across the population, then those conditions are paired with:
- Approved clinical thresholds
- Clear documentation requirements including evaluation and management
- Condition-specific expectations grounded in clinical reality
This removes ambiguity for physicians and leadership alike, and for the first time, adopts an approach that is directed at removing variation across the population, versus correcting one medical record at a time.
ClinIntell’s assessment answers a question CMOs have never been able to ask clearly:
Where is true clinical severity consistently underrepresented across our population — independent of individual charts, reviewers, or queries?
How ClinIntell Works with Physicians, and why It’s Different
A critical distinction to highlight is that ClinIntell does not operate as a retrospective, chart and revenue-driven assessment. During the assessment period:
- Physicians receive individual baseline and condition-specific performance data
- Physicians receive targeted education tied to specific high-impact conditions
- Training is grounded in approved thresholds and clinical scenarios, not coding rules
- Focus is limited to a short, high-impact list of conditions relevant to the organization’s population, and aligned with organizational goals
- Performance is measured longitudinally, across real patients in a population
This approach reduces variation by aligning physicians around approved clinical thresholds and clarifying what best documentation practices are for each of them. This eliminates guesswork and “after-the-fact” correction of the chart.
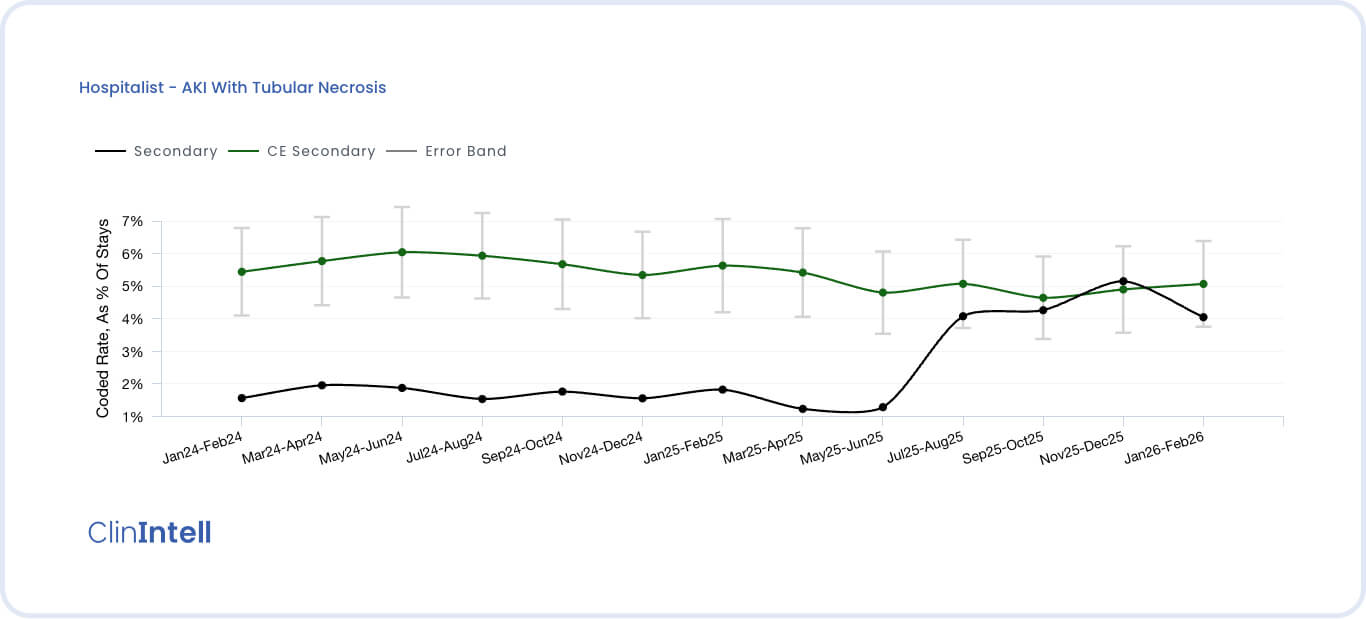
In one organization, AKI with tubular necrosis was documented inconsistently across service lines. After aligning on a single approved clinical threshold and standard, variation decreased within months, without increasing query volume.
Most importantly, improvement begins during the assessment, not after. This is an important distinction since many assessments are designed to win implementation work, delivering little value upfront.
Fewer Conditions. Less Noise. More Credibility.
Rather than overwhelming physicians with dozens of potential diagnoses and reactive queries, ClinIntell narrows focus to what actually matters clinically. For CMOs, this enables improved trust from physicians since they are now responsible for ensuring that when their patients meet specific criteria, that specific documentation practices ensure appropriate reporting on the back-end.
- Meaningful reduction in query volume
- More consistent documentation practices
- Improved trust and engagement from physicians
- Objective measurement of performance improvement
For the first time, physicians are engaged in a documentation initiative that stops being about “finding misses” and starts being about standardizing clinical representation.
Reclaiming the CMO’s Role as Physician Advocate
ClinIntell gives CMOs something they have never had before: the objective clarity on where variation is limiting severity representation across the population and whether CDI investments and initiatives have actually reduced or reinforced variation.
With this insight, CMOs can move from defending and enforcing CDI processes to leading clinical alignment and optimization, with credibility, data, and respect for physicians’ clinical judgment.
The Bottom Line
You can’t query your way to clinical truth, and you can’t fix variation by reviewing charts after the fact.
If documentation practices don’t change, CDI will continue to deliver diminishing returns, no matter how advanced the tools become.
ClinIntell’s Population-Based Assessment gives CMOs a new path forward:
- Normalize clinical signal across the population
- Reduce documentation fatigue
- Engage physicians with clarity instead of noise
- Improve how patient severity is represented, consistently and sustainably
The future of CDI is not more queries.
It is fewer conditions, clearer definitions, and accountable clinical alignment.
Schedule Your Free Population-Based Assessment





.jpg)