.svg)


Over the last decade, health systems have increasingly partnered with revenue cycle outsourcing organizations to improve operational efficiency, stabilize margins, and reduce administrative burden. These partnerships have become a core part of modern healthcare operations.
Outsourcing delivers measurable improvements in billing execution, denial management, coding workflows, and financial outcomes.
From both financial and clinical leadership perspectives, a common assumption follows: if revenue cycle is optimized, organizational performance should improve as well.
But many systems are finding that this is not the case.
Even with mature outsourcing relationships, organizations continue to face persistent challenges:
- Case mix performance plateaus despite operational improvement
- CDI query volumes remain high, amidst physician burnout
- Physician clinical thresholds and documentation standards vary widely
- Quality and financial signals appear misaligned
- Benchmark comparisons fail to explain internal variation
- Leaders lack confidence in true performance baselines
Increasingly, organizations are discovering that these issues are not revenue cycle problems. They are in fact visibility problems. And they cannot be solved through outsourcing alone.
Revenue Cycle Begins Only AFTER the Most Important Decision Is Made
Healthcare revenue cycle operations, whether internal or outsourced, function downstream of clinical care. They optimize the financial representation of what has already been documented. But every financial and quality outcome ultimately originates from one upstream event: a physician’s assessment of the patient and a clinical diagnosis being made. This occurs before coding, before CDI review, before billing, and even before benchmarking.
If patient severity is inconsistently recognized at the point of care, no level of operational excellence can fully correct the downstream effects of that costly variation. Revenue cycle improves execution. It does not evaluate diagnoses that were present but never documented. This gap represents one of the largest blind spots in healthcare performance measurement today.
The CFO Perspective: An Attribution Problem Hidden in Plain Sight
Finance leaders are trained to measure performance through operational metrics:
- Denial rates
- Clean claim percentages
- Days in accounts receivable
- Productivity benchmarks
- Cash acceleration
- Cost-to-collect
Revenue cycle outsourcing improves these indicators effectively. However, these are execution metrics.
- They answer the question: how efficiently are we processing revenue?
- They do not answer: Are we fully capturing the available clinical severity driving reimbursement AND risk adjustment?
Without visibility into diagnostic performance, CFOs face a fundamental attribution challenge. When financial performance stabilizes or plateaus, is it because:
- Revenue cycle operations are optimized, or
- Is clinical severity under-recognized?
Traditional analytics and retrospective chart reviews cannot reliably distinguish between the two. As a result, organizations may believe they have reached their performance ceiling when in reality, opportunity still exists upstream.
The CMO Perspective: Diagnostic Variation Drives Organizational Variability
From a clinical leadership standpoint, variation in diagnosis reporting is rarely intentional.
It emerges naturally from:
- Differing clinical training backgrounds
- Evolving evidence and guidelines
- Confusion around payor criteria
- Inconsistent internal clinical definitions
- Past clinical experiences
- Documentation habits formed over years of practice
Physicians caring for clinically similar patients may apply different diagnostic clinical thresholds for conditions such as:
- Electrolyte abnormalities
- Malnutrition
- Respiratory failure
- Encephalopathy
- Sepsis
For example, two physicians may treat similar patients with early sepsis. One documents “sepsis,” while the other documents only “infection.” The care may be similar, but the downstream impact on risk adjustment, quality metrics, and reimbursement is significantly different.
This is not just a documentation issue. It is a reflection of variation in clinical thresholds.
The downstream consequences are significant:
- Inconsistency in condition reporting
- Ongoing CDI queries
- Physician frustration
- Unclear clinical expectations that tie to performance metrics
- Instability in quality measures
- Misrepresentation of patient acuity, impacting reimbursement and risk adjustment
Importantly, these challenges cannot be solved solely through retrospective documentation correction, no matter who you outsource to. They originate at the moment of clinical decision-making.
Why Benchmarking Cannot Solve This Problem
Benchmarking remains a central tool in performance evaluation. It answers an important question: how do we compare to our peers?
But benchmarking cannot answer several critical questions:
- How much opportunity exists within an organization’s own population?
- Are physicians applying clinical definitions consistently?
- Are we fully recognizing and reporting patient severity?
Two hospitals with identical benchmark rankings may have dramatically different levels of unrecognized illness severity internally.
For CFOs, this creates financial uncertainty and for CMOs, it creates clinical ambiguity which inevitably fuels physician frustration.
Relative comparison of severity representation does not equal true performance measurement. Period.
Execution vs. Evaluation: Two Different Functions
Revenue cycle outsourcing and clinical severity evaluation address fundamentally different layers of performance.

These capabilities are complementary, not competitive. Outsourcing ensures efficiency. Evaluation ensures accuracy.
The Emergence of Population-Based Severity Evaluation
Healthcare has long measured nearly every operational domain such as:
- Cost accounting
- Utilization
- Productivity
- Length of stay
- Financial outcomes
- Quality performance
Yet historically, organizations lacked a way to measure clinical diagnostic performance at scale. Population-based severity evaluation introduces a new analytic layer focused on real-world physician performance rather than retrospective chart review.
This approach evaluates:
- How physicians diagnose during everyday care
- Consistency of clinical thresholds application
- Organizational patterns of severity recognition
- Opportunity that exists before CDI or coding intervention
Instead of correcting documentation after discharge, it improves alignment during care delivery itself.
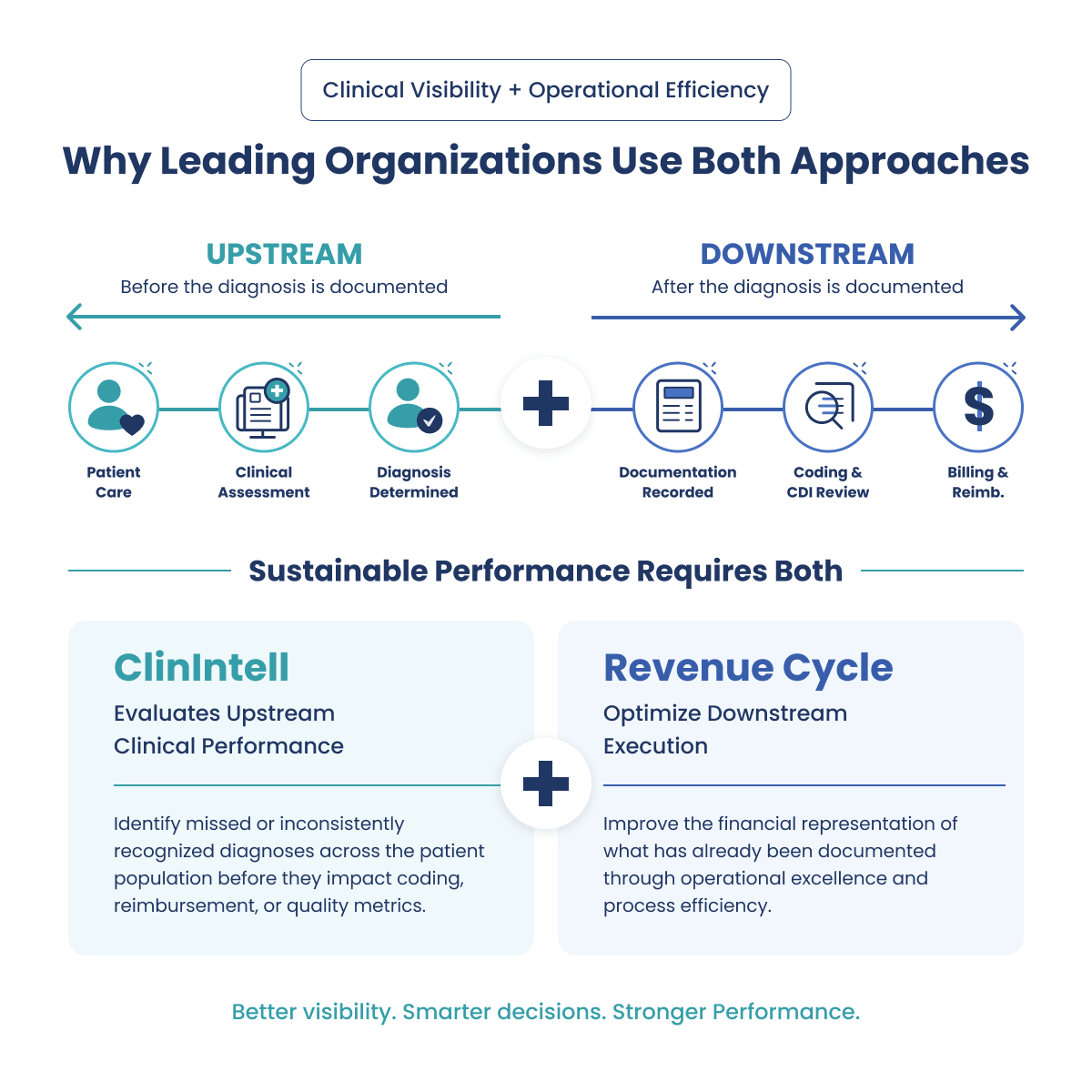
Why Leading Organizations Use Both Approaches
Health systems increasingly recognize that sustainable performance requires both operational optimization and clinical performance visibility.
Revenue cycle partners optimize downstream execution. ClinIntell evaluates upstream clinical performance, a key driver of both financial and quality outcomes. Together, organizations gain:
For CFOs
- Clearer ROI attribution
- Greater confidence in risk adjustment accuracy
- Improved forecasting reliability
- Visibility into hidden margin opportunity
- Validation of outsourcing investments
For CMOs
- Reduced diagnostic variation
- Fewer retrospective queries
- Clearer clinical expectations
- Physician alignment around clinical thresholds
- More accurate representation of patient complexity
A Shift in the Questions Leaders Are Asking
Historically, healthcare organizations asked, are we coding and billing correctly?
Today, forward-thinking leadership teams are asking a different question.
Are we, as an organization, consistently recognizing the true severity of the patients we treat?
This shift reflects a broader evolution in healthcare, from operational optimization toward clinical performance standardization and transparency.
The Future of Performance Improvement Begins Upstream
The next phase of healthcare performance will not be driven by revenue cycle alone. Value-based care demands something more: accurate, complete clinical diagnosis reporting.
Outsourcing is still necessary, but it is no longer enough. Organizations that outperform will focus upstream on the clinical decisions that drive outcomes from the start. Performance does not begin with billing. It begins with the patient.
Schedule Your Free Population-Based Assessment





